|
|
|
|
|
|
INDICATIONS |
|
ERLEADA® (apalutamide) is an androgen receptor inhibitor indicated for the treatment of patients with: |
|
|
• |
Metastatic castration-sensitive prostate cancer (mCSPC) |
|
|
• |
Non-metastatic castration-resistant prostate cancer (nmCRPC) | |
IMPORTANT SAFETY INFORMATION |
WARNINGS AND PRECAUTIONS |
|
Cerebrovascular and Ischemic Cardiovascular Events — In a randomized study (SPARTAN) of patients with nmCRPC, ischemic cardiovascular events occurred in 3.7% of patients treated with ERLEADA® and 2% of patients treated with placebo. In a randomized study (TITAN) in patients with mCSPC, ischemic cardiovascular events occurred in 4.4% of patients treated with ERLEADA® and 1.5% of patients treated with placebo. Across the SPARTAN and TITAN studies, 4 patients (0.3%) treated with ERLEADA®
and 2 patients (0.2%) treated with placebo died from an ischemic cardiovascular event. Patients with history of unstable angina, myocardial infarction, congestive heart failure, stroke, or transient ischemic attack within 6 months of randomization were excluded from the SPARTAN and TITAN studies. |
|
View Important Safety Information for ERLEADA® below. |
|
Dear , |
|
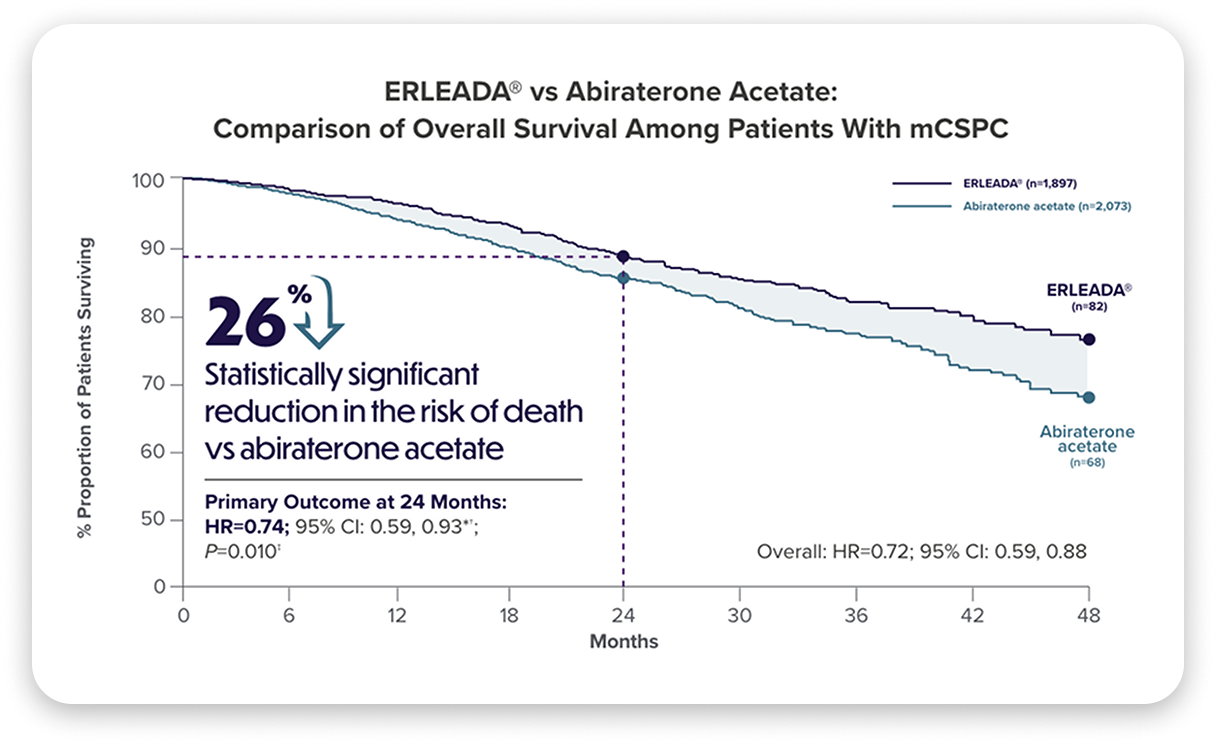
The RWE from the latest US head-to-head analysis comparing overall survival (OS) at 24 months with ERLEADA® vs abiraterone acetate in mCSPC is here. In this NEW analysis, ERLEADA® achieved a statistically significant 26% reduction in the risk of death vs abiraterone.¹ Below, you will find data from head-to-head analysis, along with information about ERLEADA® access and affordability. |
|
As you will recall, ERLEADA® + androgen deprivation therapy (ADT) was evaluated in the pivotal TITAN study that led to its approval in 2018.² |
|
|
Real-world data: OS in mCSPC¹ |
|
|
|
|
|
There have been no prospective head-to-head trials comparing the safety or efficacy of ERLEADA® to abiraterone acetate. This was a causal head-to-head analysis intended to evaluate and compare the effects of treatments on overall survival by 24 months. |
|
* |
Propensity scores were generated using probability estimates from logistic regression models using the following predictors: age (continuous), race, geographic region, payer, year of index date, time between metastasis and index date (continuous and categorical), time between PC diagnosis and index date (continuous), de novo PC, ADT use overlapping with index date, first-generation anti-androgen use, chemotherapy use, types of metastases (bone, nodal, visceral, and metastasis in multiple sites), Quan-Charlson comorbidity index (continuous), most recent PSA level (categorical), and earliest Gleason score (categorical). Each patient was attributed an inverse-probability of treatment weighting (IPTW) that was defined as follows: 1/(propensity score) for the
ERLEADA® cohort and 1/(1-propensity score) for the abiraterone acetate cohort. Normalized IPTWs were truncated at the 95th percentile.¹ | |
|
† |
A hazard ratio <1 indicates that the ERLEADA® cohort had a lower rate of death compared with abiraterone acetate cohort.¹ | |
|
‡ |
Significant at the 5% level.¹ | |
|
Data Source¹: |
|
|
• |
Clinical data from Precision Point Specialty (PPS) Analytics from community urology practices were linked with administrative claims data from the Komodo Research Database (09/17/2018 to 12/31/2023) | |
|
Study Design¹: |
|
|
• |
Primary endpoint: Evaluate survival of patients with mCSPC at 24 months after initiating ERLEADA® or abiraterone acetate |
|
|
• |
Retrospective, longitudinal, propensity score–weighted causal analysis based upon a prespecified power calculation |
|
|
• |
Patients with mCSPC were grouped into treatment cohorts based on their first dispensation or paid pharmacy claim (index date) for ERLEADA® or abiraterone acetate on or after 09/17/2019 (ERLEADA® FDA approval in mCSPC) |
|
|
• |
Inverse probability of treatment weighting (IPTW) used to account for differences in baseline characteristics between cohorts |
|
|
• |
Concurrent use of ADT was not required. Concomitant ADT use was observed in 76.8% of patients in the ERLEADA® cohort and 74.0% in the abiraterone acetate cohort |
|
|
• |
The study was designed taking into account the various guidances the FDA has issued on RWE³ |
|
|
• |
This study was not designed to assess differences in safety between cohorts | |
|
Limitations¹: |
|
|
• |
PPS represents the community urology setting and may not be representative of the entire mCSPC population in the United States |
|
|
• |
Miscoding or misclassification in clinical records or administrative claims can lead to selection and information biases despite efforts to balance the study populations |
|
|
• |
While the Komodo Research Database captured >90% of oncology-related deaths, as validated against CDC estimates, some deaths may still be missed |
|
|
• |
Abiraterone acetate is only indicated for high-risk mCSPC, which may result in residual differences relative to the ERLEADA® treatment cohort after IPTW adjustments |
|
|
• |
Regression analyses could only adjust for documented covariates, and unknown confounders may be present |
|
|
• |
Unlike Phase 3 trials assessing OS at specific events, this study evaluated survival at 24 months. Longer follow-up studies may be needed to fully assess the therapeutic effects | |
|
|
For your patients with Medicare Part D: Annual
out-of-pocket (OOP) costs for ERLEADA® may be
similar to generic abiraterone acetate and other
branded agents4,5§ |
| |
|
§ |
A patient’s actual OOP costs in 2025 are determined by their insurance plan design and coverage for their medication(s). Medicare Part D plans can offer either the standard benefit, an alternative equal in value (“actuarially equivalent”), or enhanced benefits. Some benefit designs may feature a reduced or $0 deductible and lower co-insurance and co-payments but will typically charge higher premiums, or vice versa.⁴,⁶,⁷ | |
|
CDC, U.S. Centers for Disease Control and Prevention; CI, confidence interval; FDA, U.S. Food and Drug Administration; HR, hazard ratio; mCSPC, metastatic castration-sensitive prostate cancer; PC, prostate cancer; PSA, prostate-specific antigen; RWE, real-world evidence; TITAN, Targeted Investigational Treatment Analysis of Novel Anti-androgen. | | |
|
|
WARNINGS AND PRECAUTIONS (CONTINUED) |
|
Cerebrovascular and Ischemic Cardiovascular Events (continued) — In the SPARTAN study, cerebrovascular events occurred in 2.5% of patients treated with ERLEADA® and 1% of patients treated with placebo. In the TITAN study, cerebrovascular events occurred in 1.9% of patients treated with ERLEADA® and 2.1% of patients treated with placebo. Across the SPARTAN and TITAN studies, 3 patients (0.2%) treated with ERLEADA®
and 2 patients (0.2%) treated with placebo died from a cerebrovascular event. |
|
Cerebrovascular and ischemic cardiovascular events, including events leading to death, occurred in patients receiving ERLEADA®. Monitor for signs and symptoms of ischemic heart disease and cerebrovascular disorders. Optimize management of cardiovascular risk factors, such as hypertension, diabetes, or dyslipidemia. Consider discontinuation of ERLEADA® for Grade 3 and 4 events. |
|
Fractures — In a randomized study (SPARTAN) of patients with nmCRPC, fractures occurred in 12% of patients treated with ERLEADA® and in 7% of patients treated with placebo. In a randomized study (TITAN) of patients with mCSPC, fractures occurred in 9% of patients treated with ERLEADA® and in 6% of patients treated with placebo. Evaluate patients for fracture risk. Monitor and manage patients at risk for fractures according to established treatment guidelines and consider use of bone-targeted agents. |
|
Falls — In a randomized study (SPARTAN), falls occurred in 16% of patients treated with ERLEADA® compared with 9% of patients treated with placebo. Falls were not associated with loss of consciousness or seizure. Falls occurred in patients receiving ERLEADA® with increased frequency in the elderly. Evaluate patients for fall risk. |
|
Seizure — In 2 randomized studies (SPARTAN and TITAN), 5 patients (0.4%) treated with ERLEADA® and 1 patient treated with placebo (0.1%) experienced a seizure. Permanently discontinue ERLEADA® in patients who develop a seizure during treatment. It is unknown whether anti-epileptic medications will prevent seizures with ERLEADA®. Advise patients of the risk of developing a seizure while receiving ERLEADA
® and of engaging in any activity where sudden loss of consciousness could cause harm to themselves or others. |
|
Severe Cutaneous Adverse Reactions — Fatal and life-threatening cases of severe cutaneous adverse reactions (SCARs), including Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN), and drug reaction with eosinophilia and systemic symptoms (DRESS) occurred in patients receiving ERLEADA®. |
|
Monitor patients for the development of SCARs. Advise patients of the signs and symptoms of SCARs (eg, a prodrome of fever, flu-like symptoms, mucosal lesions, progressive skin rash, or lymphadenopathy). If a SCAR is suspected, interrupt ERLEADA® until the etiology of the reaction has been determined. Consultation with a dermatologist is recommended. If a SCAR is confirmed, or for other Grade 4 skin reactions, permanently discontinue ERLEADA® [see Dosage and Administration (2.2)]. |
|
Interstitial Lung Disease (ILD)/Pneumonitis — Fatal and life-threatening interstitial lung disease (ILD) or pneumonitis can occur in patients treated with ERLEADA®. |
|
Post-marketing cases of ILD/pneumonitis, including fatal cases, occurred in patients treated with ERLEADA®. Across clinical trials (TITAN and SPARTAN, n=1327), 0.8% of patients treated with ERLEADA® experienced ILD/pneumonitis, including 0.2% who experienced Grade 3 events [see Adverse Reactions (6.1, 6.2)]. |
|
Monitor patients for new or worsening symptoms indicative of ILD/pneumonitis (eg, dyspnea, cough, fever). Immediately withhold ERLEADA® if ILD/pneumonitis is suspected. Permanently discontinue ERLEADA® in patients with severe ILD/pneumonitis or if no other potential causes of ILD/pneumonitis are identified [see Dosage and Administration (2.2)]. |
|
Embryo-Fetal Toxicity — The safety and efficacy of ERLEADA® have not been established in females. Based on findings from animals and its mechanism of action, ERLEADA® can cause fetal harm and loss of pregnancy when administered to a pregnant female. Advise males with female partners of reproductive potential to use effective contraception during treatment and for 3 months after the last dose of ERLEADA® [see Use in Specific Populations (8.1, 8.3)]
. |
ADVERSE REACTIONS |
|
The most common adverse reactions (≥10%) that occurred more frequently in the ERLEADA®-treated patients (≥2% over placebo) from the randomized placebo-controlled clinical trials (TITAN and SPARTAN) were fatigue, arthralgia, rash, decreased appetite, fall, weight decreased, hypertension, hot flush, diarrhea, and fracture. |
|
Laboratory Abnormalities — All Grades (Grade 3-4) |
|
|
• |
Hematology — In the TITAN study: white blood cell decreased ERLEADA® 27% (0.4%), placebo 19% (0.6%). In the SPARTAN study: anemia ERLEADA® 70% (0.4%), placebo 64% (0.5%); leukopenia ERLEADA® 47% (0.3%), placebo 29% (0%); lymphopenia ERLEADA® 41% (1.8%), placebo 21% (1.6%) |
|
|
• |
Chemistry — In the TITAN study: hypertriglyceridemia ERLEADA® 17% (2.5%), placebo 12% (2.3%). In the SPARTAN study: hypercholesterolemia ERLEADA® 76% (0.1%), placebo 46% (0%); hyperglycemia ERLEADA® 70% (2%), placebo 59% (1.0%); hypertriglyceridemia ERLEADA® 67% (1.6%), placebo 49% (0.8%); hyperkalemia ERLEADA®
32% (1.9%), placebo 22% (0.5%) | |
|
Rash — In 2 randomized studies (SPARTAN and TITAN), rash was most commonly described as macular or maculopapular. Adverse reactions of rash were 26% with ERLEADA® vs 8% with placebo. Grade 3 rashes (defined as covering >30% body surface area [BSA]) were reported with ERLEADA® treatment (6%) vs placebo (0.5%). |
|
The onset of rash occurred at a median of 83 days. Rash resolved in 78% of patients within a median of 78 days from onset of rash. Rash was commonly managed with oral antihistamines and topical corticosteroids, and 19% of patients received systemic corticosteroids. Dose reduction or dose interruption occurred in 14% and 28% of patients, respectively. Of the patients who had dose interruption, 59% experienced recurrence of rash upon reintroduction of ERLEADA®. |
|
Hypothyroidism — In 2 randomized studies (SPARTAN and TITAN), hypothyroidism was reported for 8% of patients treated with ERLEADA® and 1.5% of patients treated with placebo based on assessments of thyroid-stimulating hormone (TSH) every 4 months. Elevated TSH occurred in 25% of patients treated with ERLEADA® and 7% of patients treated with placebo. The median onset was at the first scheduled assessment. There were no Grade 3 or 4 adverse reactions. Thyroid replacement therapy, when clinically indicated, should be initiated or dose adjusted. |
DRUG INTERACTIONS |
|
Effect of Other Drugs on ERLEADA® — Co-administration of a strong CYP2C8 or CYP3A4 inhibitor is predicted to increase the steady-state exposure of the active moieties. No initial dose adjustment is necessary; however, reduce the ERLEADA® dose based on tolerability [see Dosage and Administration (2.2)]. |
|
Effect of ERLEADA® on Other Drugs |
|
CYP3A4, CYP2C9, CYP2C19, and UGT Substrates — ERLEADA® is a strong inducer of CYP3A4 and CYP2C19, and a weak inducer of CYP2C9 in humans. Concomitant use of ERLEADA® with medications that are primarily metabolized by CYP3A4, CYP2C19, or CYP2C9 can result in lower exposure to these medications. Substitution for these medications is recommended when possible or evaluate for loss of activity if medication is continued. Concomitant administration of ERLEADA®
with medications that are substrates of UDP-glucuronosyl transferase (UGT) can result in decreased exposure. Use caution if substrates of UGT must be co-administered with ERLEADA® and evaluate for loss of activity. |
|
P-gp, BCRP, or OATP1B1 Substrates — Apalutamide is a weak inducer of P-glycoprotein (P-gp), breast cancer resistance protein (BCRP), and organic anion transporting polypeptide 1B1 (OATP1B1) clinically. Concomitant use of ERLEADA® with medications that are substrates of P-gp, BCRP, or OATP1B1 can result in lower exposure of these medications. Use caution if substrates of P-gp, BCRP, or OATP1B1 must be co-administered with ERLEADA® and evaluate for loss of activity if medication is continued. |
|
Please see full Prescribing Information for ERLEADA®. |
|
cp-50507v7 | |
| |
|
|
|
If you would like to learn more about ERLEADA®, please visit our website at ErleadaHCP.com. |
|
Thank you. |
|
Johnson & Johnson |
|
References: |
|
1. |
Lowentritt B, Bilen MA, Khilfeh I, et al. Overall survival in patients with metastatic castration sensitive prostate cancer treated with apalutamide versus abiraterone acetate – a head-to-head analysis of real-world patients in the United States. Poster presented at: 2024 European Congress of Oncology Pharmacy; October 2-4, 2024; Lisbon, Portugal. | |
|
2. |
ERLEADA® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc. | |
|
|
|
|
|
5. |
Data on file. Janssen Biotech, Inc. | |
|
|
|
|
|
Please do not reply to this email address as it is not set up to process any responses. |
|
| |
| |
|
|
|
|
|
Janssen Biotech, Inc., a Johnson & Johnson company |
|
800 Ridgeview Drive |
|
Horsham, PA 19044 |
|
© Johnson & Johnson and its affiliates 2025 02/25 cp-499699v1 | |
| |
|
| | |  |