|
Central Nervous System (CNS) Effects: A broad spectrum of CNS effects can
occur; overall, CNS effects occurred in 52% of the 476 patients receiving LORBRENA. These included
seizures (1.9%, sometimes in conjunction with other neurologic findings), psychotic effects (7%;
0.6% severe [Grade 3 or 4]), and changes in cognitive function (28%; 2.9% severe), mood (including
suicidal ideation) (21%; 1.7% severe), speech (11%; 0.6% severe), mental status (1.3%; 1.1% severe),
and sleep (12%). Median time to first onset of any CNS effect was 1.4 months (1 day to 3.4 years).
Overall, 2.1% and 10% of patients required permanent or temporary discontinuation of LORBRENA,
respectively, for a CNS effect; 8% required dose reduction. Withhold and resume at same or reduced
dose or permanently discontinue based on
severity.
Hyperlipidemia: Increases in serum cholesterol and
triglycerides can occur. Grade 3 or 4 elevations in total cholesterol occurred in 18% and Grade 3 or
4 elevations in triglycerides occurred in 19% of the 476 patients who received LORBRENA. Median time
to onset was 15 days for both hypercholesterolemia and hypertriglyceridemia. Approximately 4% and 7%
of patients required temporary discontinuation and 1% and 3% of patients required dose reduction of
LORBRENA for elevations in cholesterol and in triglycerides in Study B7461001 and Study B7461006,
respectively. Eighty-three percent of patients required initiation of lipid-lowering medications,
with a median time to onset of start of such medications of 17 days. Initiate or increase the dose
of lipid-lowering agents in patients with hyperlipidemia. Monitor serum cholesterol and
triglycerides before initiating LORBRENA, 1 and 2 months after initiating LORBRENA, and periodically
thereafter. Withhold and resume at same dose for the first occurrence; resume at same or reduced
dose of LORBRENA for recurrence based on severity.
Atrioventricular (AV)
Block: PR interval
prolongation and AV block can occur. In 476 patients who received LORBRENA at a dose of 100 mg
orally once daily and who had a baseline electrocardiography (ECG), 1.9% experienced AV block and
0.2% experienced Grade 3 AV block and underwent pacemaker placement. Monitor ECG prior to initiating
LORBRENA and periodically thereafter. Withhold and resume at reduced or same dose in patients who
undergo pacemaker placement. Permanently discontinue for recurrence in patients without a
pacemaker.
Interstitial Lung Disease (ILD)/Pneumonitis: Severe or life-threatening pulmonary
adverse reactions consistent with ILD/pneumonitis can occur. ILD/pneumonitis occurred in 1.9% of
patients, including Grade 3 or 4 ILD/pneumonitis in 0.6% of patients. Four patients (0.8%)
discontinued LORBRENA for ILD/pneumonitis. Promptly investigate for ILD/pneumonitis in any patient
who presents with worsening of respiratory symptoms indicative of ILD/pneumonitis (e.g., dyspnea,
cough, and fever). Immediately withhold LORBRENA in patients with suspected ILD/pneumonitis.
Permanently discontinue LORBRENA for treatment-related ILD/pneumonitis of any
severity.
Hypertension: Hypertension can occur. Hypertension
occurred in 13% of patients, including Grade 3 or 4 in 6% of patients. Median time to onset of
hypertension was 6.4 months (1 day to 2.8 years), and 2.3% of patients temporarily discontinued
LORBRENA for hypertension. Control blood pressure prior to initiating LORBRENA. Monitor blood
pressure after 2 weeks and at least monthly thereafter. Withhold and resume at reduced dose or
permanently discontinue based on severity.
Hyperglycemia: Hyperglycemia can occur. Hyperglycemia
occurred in 9% of patients, including Grade 3 or 4 in 3.2% of patients. Median time to onset of
hyperglycemia was 4.8 months (1 day to 2.9 years), and 0.8% of patients temporarily discontinued
LORBRENA for hyperglycemia. Assess fasting serum glucose prior to initiating LORBRENA and monitor
periodically thereafter. Withhold and resume at reduced dose or permanently discontinue based on
severity.
Embryo-fetal Toxicity: LORBRENA can cause fetal harm. Advise
pregnant women of the potential risk to a fetus. Advise females of reproductive potential to use an
effective non-hormonal method of contraception, since LORBRENA can render hormonal contraceptives
ineffective, during treatment with LORBRENA and for at least 6 months after the final dose. Advise
males with female partners of reproductive potential to use effective contraception during treatment
with LORBRENA and for 3 months after the final dose.
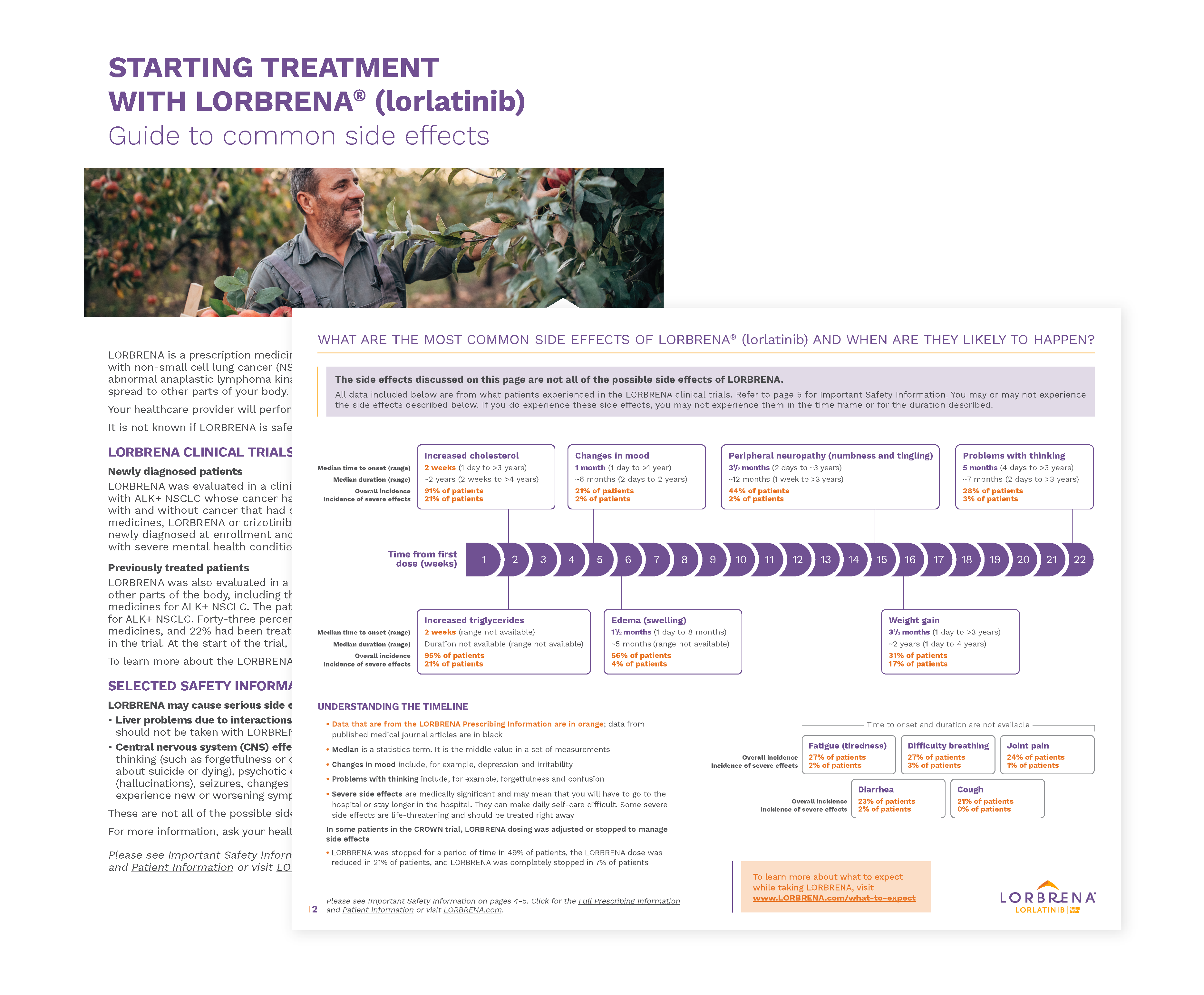
Adverse
Reactions: In the pooled
safety population of 476 patients who received 100 mg LORBRENA once daily, the most frequent (≥ 20%)
adverse reactions were edema (56%), peripheral neuropathy (44%), weight gain (31%), cognitive
effects (28%), fatigue (27%), dyspnea (27%), arthralgia (24%), diarrhea (23%), mood effects (21%),
and cough (21%). The most frequent (≥ 20%) Grade 3-4 laboratory abnormalities in patients receiving
LORBRENA were hypercholesterolemia (21%) and hypertriglyceridemia (21%).
In previously
untreated patients, serious adverse reactions occurred in 34% of the 149 patients treated with
LORBRENA; the most frequently reported serious adverse reactions were pneumonia (4.7%), dyspnea
(2.7%), respiratory failure (2.7%), cognitive effects (2.0%), and pyrexia (2.0%). Fatal adverse
reactions occurred in 3.4% of patients and included pneumonia (0.7%), respiratory failure (0.7%),
cardiac failure acute (0.7%), pulmonary embolism (0.7%), and sudden death (0.7%). In the Phase 1/2
study, serious adverse reactions occurred in 32% of the 295 patients; the most frequently reported
serious adverse reactions were pneumonia (3.4%), dyspnea (2.7%), pyrexia (2%), mental status changes
(1.4%), and respiratory failure (1.4%). Fatal adverse reactions occurred in 2.7% of patients and
included pneumonia (0.7%), myocardial infarction (0.7%), acute pulmonary edema (0.3%), embolism
(0.3%), peripheral artery occlusion (0.3%), and respiratory distress
(0.3%).
Drug Interactions: LORBRENA is contraindicated in patients
taking strong CYP3A inducers. Avoid concomitant use with moderate CYP3A inducers, strong CYP3A
inhibitors, and fluconazole. If concomitant use of moderate CYP3A inducers cannot be avoided,
increase the LORBRENA dose as recommended. If concomitant use with a strong CYP3A inhibitor or
fluconazole cannot be avoided, reduce the LORBRENA dose as recommended. Avoid concomitant use of
LORBRENA with CYP3A substrates and P-gp substrates, which may reduce the efficacy of these
substrates.
Lactation: Because of the potential for serious
adverse reactions in breastfed infants, instruct women not to breastfeed during treatment with
LORBRENA and for 7 days after the final dose.
Hepatic
Impairment: No dose
adjustment is recommended for patients with mild hepatic impairment. The recommended dose of
LORBRENA has not been established for patients with moderate or severe hepatic
impairment.
Renal Impairment: Reduce the dose of LORBRENA for
patients with severe renal impairment. No dose adjustment is recommended for patients with mild or
moderate renal impairment.
Please see Full
Prescribing Information.
|